10 Things You Might Not Know About Decompression Illness (DCI)
Remember that the term decompression illness (DCI) includes both decompression sickness (DCS) resulting from dissolved nitrogen (or another inert gas) being eliminated from a diver’s body tissues; and arterial gas embolism (AGE) which is caused by air entering the arterial blood as a result of a burst lung.
DCI was first reported in 1667 in a snake – not a diver!
Boyle (from Boyle’s Law) placed a viper in a vacuum and noticed a bubble forming in its eye.
It’s possible to get a burst lung and subsequent DCI (arterial gas embolism) in as little as 1.2 metres of water
If a diver fills his lungs with compressed air and surfaces without exhaling, there is enough pressure change in the first 1.2 metres from the surface to over-expand the lungs sufficiently to cause a tear.
Divers have suffered from DCS after ascending from depths as shallow as about 6-7 metres
It used to be thought that one had to dive deeper than 10 metres before DCS was a risk, but this is now known to be untrue.

Most divers (possibly around 90 percent) who get DCI have been diving within the limits of their dive computer or tables
However, the risk of DCI increases when a diver exceeds these limits. This indicates that the limits cannot accurately account for individual differences between divers and the various factors that can influence nitrogen uptake and elimination during a dive. All divers should add conservatism to their decompression calculations, especially if the diving is purely recreational and dive time doesn’t need to be maximised.
Bubbles form within divers’ bodies during or after many dives, especially repetitive and deeper dives
These bubbles can be detected using ultrasound and usually do not cause symptoms. Some divers “bubble” more than others. A slow ascent rate and doing a safety stop reduces the amount of bubbling and therefore the risk of DCI.
Some divers are more susceptible to DCI than others
Divers with a patent foramen ovale (PFO),which is a common heart defect that can enable blood to flow across the heart, have a significantly higher risk of DCI (sometimes quoted as two to eight times, depending on the size of the hole). Other factors such as being overweight, increasing age, lack of fitness and dehydration may also play a role although there is little hard evidence to support some of these beliefs.
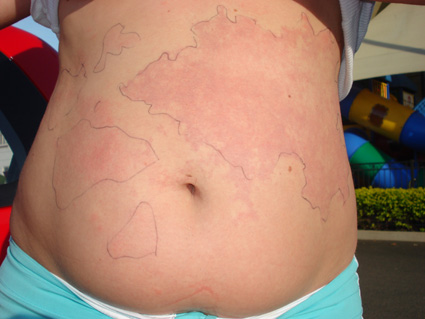
A mottled reddish/purple/bluish rash is an increasingly common sign of DCI and is often associated with the presence of a PFO
Skin-related DCI used to be relatively uncommon in recreational divers. However, over more recent years it has become far more common. Part of the reason for this could be the result of the more frequent and longer dives and shorter surface intervals enabled by dive computers.
Oxygen first aid is often delayed, given using unsuitable equipment and for too short a period
Good oxygen first aid is very important in the management of DCI and this is often poorly done. To maximise the benefit, near-100 percent oxygen should be given from the time symptoms first occur, and continued until a diving doctor advises that it be stopped.
Many dive operators in remote areas do not have access to a sufficient supply of oxygen to last until an injured divers receives appropriate medical care
It can sometimes take over 24 hours for an evacuation team to reach some remote locations, so a large supply of oxygen is required. Check this out before you go on a dive trip to an area without good access to suitable medical care.
About 800 divers are treated for DCI in the Asia-Pacific each year
—
By DAN AP’s John Lippmann
Check out this incredible offer from DAN Asia-Pacific and UW360:
1 YEAR DAN Asia-Pacific Membership + 1 YEAR Subscription to Scuba Diver AUSTRALASIA + OCEAN PLANET Want to get your hands on this package? Click here.
You may also like




